Reports
20 Years of Complement Inhibition in PNH: Lessons from the Past, Hope for the Future
This report is based on medical evidence presented at sanctioned medical congress, from peer reviewed literature or opinion provided by a qualified healthcare practitioner. The consumption of the information contained within this report is intended for qualified Canadian healthcare practitioners only.
PRIORITY PRESS - EHA2022 Hybrid – European Hematology Association (EHA)
In-person/virtual, Vienna, Austria / June 9–12, 2022
In-person/Virtual – Although paroxysmal nocturnal hemoglobinuria (PNH) is a rare and often under-appreciated disease, this year’s EHA hybrid meeting featured a diverse range of presentations on the topic. Two satellite symposia reviewed the pathophysiology and diagnosis of PNH and gave insights into the burden of disease and the experience with established and novel treatment options. A further 25 posters, presentations, and virtual thematic sessions covered new information about PNH biology, real-world and clinical data for current gold-standard therapies eculizumab and ravulizumab, and clinical trial analyses for emerging therapeutic options.
Chief Medical Editor: Dr. Léna Coïc, Montréal, Quebec
“We’re privileged to have 20 years of experience with complement inhibition in PNH – it’s 20 years almost to the day since the first patient was treated with eculizumab in the pivotal trial in May 2002,” said Dr. Austin Kulasekararaj, head of the PNH Centre, King’s College Hospital, London, UK.1 PNH is a rare, chronic, and often progressive condition characterized by intravascular hemolysis, thrombosis, and organ damage caused by uncontrolled activation of terminal complement. Over the course of EHA2022, expert presenters built on those two decades of experience and knowledge to provide new insights into the burden of PNH and the role of complement inhibition for managing the disease and improving patients’ lives.
Unmet Needs in PNH: Diagnostic Delays and the Burden of Disease and Treatment
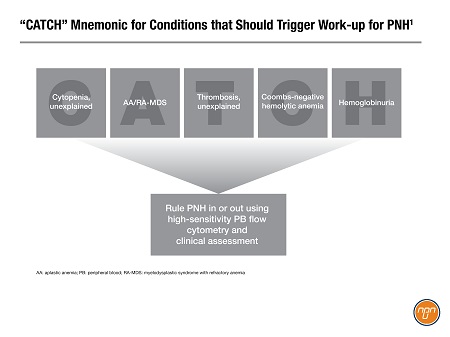
“PNH patients are really unique in their presentations and always a challenge,” said Dr. Alexander Röth, Professor, University Hospital, Essen, Germany, during a satellite symposium about the lessons learned from 20 years of complement inhibitor therapies.1 Dr. Christopher Patriquin, Assistant Professor, University Health Network, Toronto, and Chair, Canadian PNH Network, described “the classic clinical triad that you will always see in a review paper on PNH: direct antiglobulin test (DAT)-negative hemolysis, thrombophilia, and marrow failure,” but added that, “More commonly, patients will present with unexplained fatigue, chest pain and dyspnea, abdominal pain, renal involvement, and smooth muscle dystonic symptoms. And it’s this diversity and range of presentations that can often lead to the delay in diagnosis for these patients.”1 To help clinicians diagnose PNH more promptly, Dr. Patriquin highlighted the “CATCH” mnemonic developed by the Canadian PNH Network, which describes five clinical scenarios that should trigger suspicion of PNH and appropriate work-up with physical exam and flow cytometry (Figure 1).1
Figure 1.
Difficulties and delays in diagnosing PNH were also explored in a symposium on unmet needs in PNH, including the patient perspective.2 When asked about her diagnosis journey, Alex Naylor, a patient from the UK, said, “It was a very stressful time, a very anxious time. And really, it was about learning that what I had come to believe was just the way I lived, was actually a set of symptoms for a disease.”2
Evolving the Standard of Care
“Effective therapy for PNH needs to ensure that terminal complement is well inhibited, regardless of the molecular target,” said Dr. Patriquin.1 Based on its effective inhibition of the terminal complement component C5 and its robust clinical safety and efficacy profile, eculizumab has become established over the last 20 years as the standard of care for PNH; its longer-acting derivative ravulizumab is now starting to move into the first-line position in countries where it has been approved.
Summarizing the trial and clinical experience to date with ravulizumab, Dr. Kulasekararaj said, “It's fantastic for patients because it's given every eight weeks, it definitely abolishes pharmacokinetic-mediated breakthrough hemolysis and it's non-inferior to eculizumab.”1 Since ravulizumab has been available for about two years in some countries, studies of real-world clinical use are now able to evaluate the impact of switching from eculizumab. Dr. Alicia Rovó and her colleagues involved in a Swiss PNH registry reported on 56 patients who switched to ravulizumab in 2020. After a median follow-up of 27 months, patients experienced an increase in mean hemoglobin from 63 ± 47 g/L at baseline to 105 ± 25 g/L at last visit. After a year of ravulizumab, mean levels of the key hemolysis marker lactate dehydrogenase (LDH) decreased from 1457 ± 706 U/L to 403 ± 212 U/L and 91% of patients were transfusion-free, compared to 50% at baseline. The authors highlighted that ravulizumab has been rapidly adopted since its approval and that it “may likely become the new standard of care for patients with PNH.”3
Dr. Kulasekararaj and co-investigators reported on a pooled analysis of survival data across the ravulizumab clinical development program. Out of 475 patients and a total of 1479.0 patient-years of exposure, there were only 12 deaths, for an incidence of 0.8 per 100 patient-years. Half the deaths were due to infection or sepsis and the remainder to neoplasms, cardiac disorders, or respiratory disorders. The authors concluded that the low rates of infection and death support the long-term use of ravulizumab for PNH.4
Although the convenience of C5 inhibitor therapy has improved with ravulizumab’s dosing every 8 weeks compared to eculizumab’s administration every 2 weeks, many patients still find it burdensome to go to a clinic for their intravenous (IV) doses. Subcutaneous (SUBQ) dosing has the potential to reduce the number of clinic visits and allow patients to manage their therapy at home. A SUBQ formulation of ravulizumab administered once weekly via an on-body delivery system is currently in clinical development (not yet commercially available in Canada). In their poster at EHA2022, Dr. Mustafa Yenerel and colleagues reported that the SUBQ formulation maintained efficacy and improved patient satisfaction compared to the IV formulation.5
Expanding Our Understanding of Newer Therapeutic Options
Pegcetacoplan is an inhibitor of the proximal complement component C3, now approved in several countries (though not yet in Canada) for patients whose PNH does not adequately respond to eculizumab or ravulizumab. Several additional analyses of its phase 2 and 3 trials were reported at EHA2022.
In an oral presentation, Dr. David Gómez-Almaguer, Professor, Universidad Autonoma de Nuevo León, Mexico, said that pegcetacoplan provided significant improvements in patient-reported quality of life (EORTC QLQ-C30, LASA, and FACIT-Fatigue scales) and in fatigue and dyspnea in treatment-naïve patients.6 A poster from Dr. Raymond Wong and colleagues demonstrated that treatment-naïve patients in the control arm of the phase 3 PRINCE trial who experienced acute declines in hemoglobin could be effectively rescued with pegcetacoplan7, while an analysis across three core trials showed that pegcetacoplan could bring hematologic (hemoglobin, LDH) and quality-of-life parameters back into the normal range for patients with less profound anemia at baseline (≥10 g/dL).8
Based on the pegcetacoplan data and the phase 2 findings for danicopan and iptacopan, two other novel inhibitors of proximal complement (not yet available in Canada), the speakers in the unmet needs symposium were enthusiastic about having another potential therapeutic target in patients whose PNH does not respond adequately to C5 inhibition. However, Dr. Régis Peffault de Latour, Professor, Saint-Louis Hospital, Paris, France, advised clinicians to be vigilant for infectious complications, since long-term blockade of proximal complement could theoretically reduce the body’s defense against pathogens such as Streptococcus pneumoniae. He concluded, “This is a reason why we should follow our patients outstandingly carefully - not only clinically speaking, but also at the PK/PD [pharmacokinetic/pharmacodynamic] level long-term.”2
Conclusions
PNH is a rare and under-appreciated disease that can place a significant burden on patients. Ravulizumab is starting to replace eculizumab as the standard of care and real-world data are emerging to support its robust safety and efficacy profile from clinical trials. A subcutaneous formulation of ravulizumab is being developed that may improve patient satisfaction while maintaining the efficacy of the intravenous version. Proximal complement inhibition is a novel therapeutic strategy that holds promise in patients whose PNH is not adequately managed with C5 inhibitors, although increased risk of infection may be a concern.
References:
1. Kulasekararaj A, et al. What we have learned from the last 20 years of complement inhibition in PNH. Satellite symposium at EHA2022 Hybrid, June 9, 2022.
2. Peffault de Latour R, et al. Unmet needs and future possibilities for PNH: Hear the patient perspective and expert opinions. Satellite symposium at EHA2022 Hybrid, June 11, 2022.
3. Rovó A, et al. Real-world evidence of safety and effectiveness of eculizumab and switch to ravulizumab in a Swiss patient population with paroxysmal nocturnal hemoglobinuria. EHA2022 Hybrid June 9-17, 2022. Poster P834.
4. Kulasekararaj A, et al. Long-term complement inhibition and survival outcomes in patients with paroxysmal nocturnal hemoglobinuria: an interim analysis of the ravulizumab clinical trials. EHA2022 Hybrid June 9-17, 2022. Poster P812.
5. Yenerel M, et al. Efficacy, treatment administration satisfaction and safety of subcutaneous ravulizumab through 1 year in patients with paroxysmal nocturnal hemoglobinuria who received prior intravenous eculizumab. EHA2022 Hybrid June 9-17, 2022. Poster P813.
6. Gómez-Almaguer D, et al. Effect of pegcetacoplan on quality of life in complement-inhibitor naïve patients with paroxysmal nocturnal hemoglobinuria: results from the phase 3 PRINCE study. EHA2022 Hybrid June 9-17, 2022. Oral presentation S303.
7. Wong R, et al. Pegcetacoplan rapidly stabilizes complement inhibitor naïve patients with paroxysmal nocturnal hemoglobinuria experiencing hemolysis with acute hemoglobin decreases; prince trial post hoc analysis. EHA2022 Hybrid June 9-17, 2022. Poster P838.
8. Panse J, et al. Normalization of hematologic and health-related quality of life markers in patients with paroxysmal nocturnal hemoglobinuria treated with pegcetacoplan and baseline hemoglobin at or above 10 g/dL. EHA2022 Hybrid June 9-17, 2022. Poster P828.